 Skip to content
Skip to content
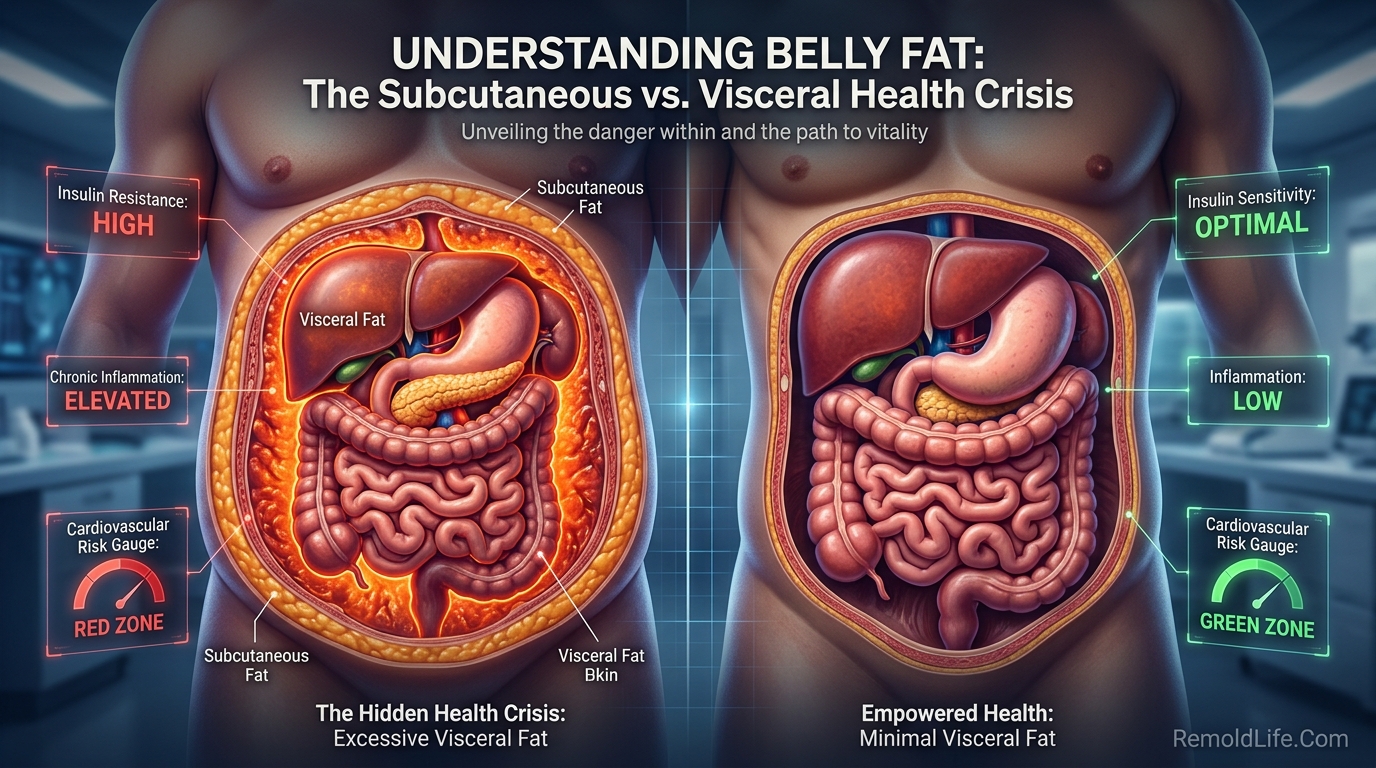
If you want to know how to lose belly fat, the first thing worth establishing is what belly fat actually is — because there are two types, they have very different health implications, and understanding the difference matters for addressing the right one.
Subcutaneous fat sits directly under the skin — it’s the fat you can pinch. It’s the type most people are thinking about aesthetically, and while excess amounts aren’t ideal, it’s less metabolically dangerous than the other kind.
Visceral fat surrounds your internal organs in the abdominal cavity. You can’t see or pinch it directly — it sits deeper. This is the fat that research consistently links to type 2 diabetes, cardiovascular disease, insulin resistance, and chronic inflammation. Reducing visceral fat has dramatic health benefits even when the change on the scale is modest.
Most advice about “losing belly fat” conflates both types. This guide distinguishes them and focuses on evidence-based strategies for both.
Why You Can’t Spot-Reduce Belly Fat
Before getting into what works, one important clarification: spot reduction — the idea that you can specifically target fat loss in one body area through exercise that works that area — is a myth with no credible scientific support.
Doing hundreds of crunches doesn’t specifically reduce belly fat. Crunches strengthen the abdominal muscles underneath the fat, but fat loss happens systemically — your body decides where to draw from based on genetics, hormones, and overall energy balance, not which muscles you’re working.
This matters because it shifts the focus from exercise type to overall approach — which is what the research actually supports.
What Drives Belly Fat Accumulation
Several factors specifically promote abdominal fat storage:
Caloric surplus over time — the fundamental driver of fat gain. When you consistently consume more calories than you expend, the excess is stored as fat — and genetics largely determines where it goes first.
Chronically elevated cortisol — the stress hormone cortisol specifically promotes visceral fat accumulation. The mechanism involves cortisol directing fat storage toward the abdominal region and promoting fat cell growth in the visceral area. This is why chronic stress is associated with abdominal weight gain independent of caloric intake.
Poor sleep — sleep deprivation increases cortisol, reduces leptin (satiety hormone), and raises ghrelin (hunger hormone) — producing a hormonal environment that promotes fat storage, particularly in the abdominal area.
Excess sugar and refined carbohydrates — high fructose intake specifically promotes visceral fat. Research published in Obesity found that fructose-sweetened beverages were associated with significantly greater visceral fat accumulation than glucose-sweetened ones.
Alcohol — the term “beer belly” isn’t entirely mythology. Regular alcohol consumption — particularly heavy drinking — is associated with greater visceral fat. Alcohol delivers calories with no nutritional value, promotes fat storage, disrupts liver metabolism, and increases cortisol.
Declining estrogen in women — menopause shifts fat distribution toward the abdominal region, which is why many women notice increased belly fat during this transition even without significant weight change.
Genetics — where your body tends to store fat first is significantly genetically determined. Some people store fat preferentially in the abdominal area; others in the hips and thighs. You can’t change the predisposition, but you can reduce total body fat.
What the Research Shows Actually Works

1. A Sustainable Caloric Deficit Through Diet
Fat loss requires consuming fewer calories than you expend over time. There’s no workaround for this fundamental principle — not intermittent fasting, not specific foods, not particular workout types. The question is how to create and maintain a caloric deficit sustainably.
A modest deficit of 300–500 calories per day produces approximately 0.3–0.5 kg of fat loss per week — which is sustainable and doesn’t trigger the aggressive hunger and metabolic adaptation that comes with severe restriction.
What a sustainable deficit looks like in practice:
- Reducing portion sizes of energy-dense foods (oils, refined grains, processed snacks)
- Replacing calorie-dense, low-satiety foods with high-volume, high-fiber options
- Reducing alcohol significantly
- Eliminating liquid calories (sugary drinks, juice, alcohol)
2. Reduce Added Sugar and Refined Carbohydrates
Beyond pure caloric impact, reducing added sugar and refined carbohydrates specifically reduces visceral fat through hormonal mechanisms — primarily by lowering insulin levels, which promotes fat release from adipose tissue.
A study published in the Annals of Internal Medicine found that a low-carbohydrate diet produced significantly greater visceral fat reduction than a low-fat diet — even with similar total caloric deficits. The hormonal environment created by lower carbohydrate and insulin levels appears to preferentially mobilize visceral fat.
Practical changes:
- Replace sugary drinks with water, unsweetened tea, or black coffee
- Reduce refined grain products (white bread, white rice, pastries) in favor of vegetables, legumes, and whole grains
- Reduce added sugar in general — checking labels helps identify hidden sugar in sauces, condiments, and packaged foods
3. Increase Protein Intake
Higher protein intake supports fat loss in multiple ways: it increases satiety (reducing overall caloric intake), has a higher thermic effect (burns more calories in digestion), preserves muscle mass during a caloric deficit, and reduces the hormonal responses that drive fat storage.
Research published in The American Journal of Clinical Nutrition found that higher protein diets produced greater fat loss and better preservation of lean mass compared to lower protein diets at the same caloric intake.
A practical target: 1.6–2.0 grams of protein per kilogram of body weight daily. Sources: lean meat, fish, eggs, dairy, legumes, tofu.
4. Aerobic Exercise — Particularly at Moderate Intensity
Aerobic exercise is more effective than resistance training alone for visceral fat reduction — this is consistent across multiple studies. A meta-analysis published in PLOS ONE found that aerobic exercise produced significantly greater visceral fat reduction than resistance training, though both produce benefits.
The mechanism: aerobic exercise mobilizes fatty acids from visceral fat tissue during and after activity, and the cardiovascular and hormonal changes from regular aerobic activity shift the body’s fat storage balance over time.
Effective options: brisk walking, running, cycling, swimming, rowing. Consistency matters more than intensity — moderate-intensity aerobic exercise done regularly outperforms occasional high-intensity sessions.
Target: 150–300 minutes of moderate aerobic activity per week. Research suggests the upper end of this range (closer to 300 minutes) produces significantly more visceral fat reduction than the lower end.
5. Add Resistance Training to Preserve Muscle
While aerobic exercise is superior for direct visceral fat reduction, resistance training is important for body composition. During a caloric deficit, the body can lose muscle alongside fat — resistance training minimizes this loss.
More muscle also means higher resting metabolic rate — which supports maintaining a caloric deficit without increasingly severe restriction. Two to three resistance training sessions per week alongside regular aerobic exercise is the combination most supported by evidence for both fat loss and body composition improvement.

6. Manage Cortisol and Chronic Stress
Because cortisol specifically promotes visceral fat, managing chronic stress is not optional for people struggling specifically with abdominal fat. This includes:
- Regular stress management practices (exercise, mindfulness, social connection)
- Protecting sleep (8 hours, consistent schedule, sleep environment)
- Addressing sources of chronic stress rather than only managing symptoms
The effectiveness of stress management for visceral fat reduction is sometimes underestimated because it’s harder to quantify than diet and exercise changes. But for people under significant chronic stress, addressing it can be as impactful as dietary changes.
7. Prioritize Sleep
As covered, poor sleep promotes visceral fat through multiple hormonal mechanisms. Research from the University of Chicago found that reducing sleep from 8.5 hours to 5.5 hours for two weeks cut the proportion of weight loss from fat in half — the sleep-deprived group lost more muscle and less fat even on the same diet.
Protecting sleep isn’t a “nice to have” when trying to lose belly fat — it’s integral to the process.
Approaches That Don’t Work (Despite Popular Claims)
Ab exercises for spot reduction — as explained above, no evidence.
“Fat burning” supplements — the vast majority have no credible evidence. A few (caffeine, green tea extract) have very modest effects on metabolism — not meaningful for fat loss without diet and exercise changes.
Juice cleanses and detoxes — no evidence for fat loss; may cause temporary water weight loss.
Very low-calorie diets — severe caloric restriction (below 800 calories) causes significant muscle loss, metabolic adaptation, and is rarely sustainable. The body’s response to severe restriction actively resists continued fat loss.
Waist trainers and body wraps — produce temporary water loss and surface compression; no evidence for fat reduction.
Realistic Timeline for Belly Fat Reduction
Consistency and patience matter. With a sustainable approach:
| Approach | Expected Visceral Fat Reduction | Timeline |
|---|---|---|
| Dietary changes alone (500 cal deficit) | 0.3–0.5 kg/week total fat loss | 3–6 months for meaningful change |
| Aerobic exercise 5x/week | Additional 5–10% visceral fat reduction | 8–12 weeks |
| Combined diet + exercise + stress management | Maximum sustainable results | 3–6+ months |
Visceral fat is often among the first fat reserves to reduce with a caloric deficit — which is good news for health outcomes even before significant aesthetic change.
Frequently Asked Questions
The fat itself is the same, but the mechanisms driving its accumulation differ. Stress-driven visceral fat involves cortisol-mediated preferential storage in the abdominal region. Addressing the cortisol component (stress management, sleep) is particularly important for people whose belly fat accumulation correlates strongly with stress periods.
Directly, no. Adequate hydration supports metabolism generally and can reduce water retention (which affects appearance), and drinking water before meals modestly reduces caloric intake. But water itself doesn’t specifically reduce adipose tissue.
Research generally favors lower-carbohydrate approaches for specifically reducing visceral fat — the hormonal environment of lower insulin levels appears to preferentially mobilize abdominal fat. However, the most important factor is sustained caloric deficit, not the specific macronutrient ratio. The best diet is the one you can sustain over months.
The National Institutes of Health identifies waist circumference as a practical screening tool: above 35 inches for women and 40 inches for men is associated with significantly increased cardiovascular and metabolic risk. Waist-to-height ratio (waist circumference divided by height) above 0.5 is another practical benchmark. These aren’t absolute thresholds — risk increases continuously, not at a specific cutoff.
Intermittent fasting can be an effective way to create a caloric deficit, and some studies show specific benefits for visceral fat reduction through mechanisms including improved insulin sensitivity and increased fat oxidation during fasting windows. A 2020 review in Obesity Reviews found intermittent fasting effective for visceral fat reduction, though not significantly more effective than continuous caloric restriction when calories are matched.

Final Thoughts
Losing belly fat — particularly the visceral type that affects metabolic health — requires the same things that support overall health: consistent caloric deficit through improved diet, regular aerobic exercise, adequate sleep, and stress management. There are no shortcuts that bypass these fundamentals.
The good news is that visceral fat responds well to lifestyle change and is often among the first fat reserves mobilized when you create a sustainable caloric deficit. The changes that reduce it are the same changes that reduce risk for heart disease, type 2 diabetes, and other chronic conditions — so the health return is broader than the aesthetic one.
For related reading, type 2 diabetes prevention covers the metabolic health connection between visceral fat and blood sugar, and how to manage stress and anxiety addresses the cortisol component that many people overlook.
Sources:
- National Heart, Lung, and Blood Institute — Waist Circumference and Health Risk: https://www.nhlbi.nih.gov/
- Hairston KG et al. — “Lifestyle Factors and 5-Year Abdominal Fat Accumulation.” Obesity (2012)
- Drenowatz C et al. — Aerobic Exercise and Visceral Fat. PLOS ONE Meta-Analysis
- Sacks FM et al. — “Comparison of Weight-Loss Diets.” NEJM (2009)
- Nedeltcheva AV et al. — Sleep and Fat Loss, Annals of Internal Medicine (2010)